
Clinical Care
Highly Specialized Care for ALS Patients –
Outpatient and Inpatient Services
he Department of Neurology at Ulm University Hospital specializes in the care of patients with ALS in both outpatient and inpatient settings. With more than 400 inpatient and outpatient cases per year, the center serves a wide regional and supraregional catchment area.
Patients are referred for: initial diagnosis (including expert consultation for first diagnosis or second opinions), regular follow-up assessments, participation in clinical trials (see section on studies), initiation of non-invasive ventilation, placement of a PEG feeding tube and management of complications during the course of the disease, such as acute deterioration (particularly respiratory decline).
We optimize existing non-invasive or invasive home ventilation and support the transition from non-invasive to invasive ventilation when required.
All relevant diagnostic and therapeutic procedures are available. Inpatient care is provided by a multidisciplinary team including physicians, specialized nursing staff, therapists (respiratory therapy, speech and language therapy, physiotherapy, occupational therapy, nutritional therapy), and social services.
Ventilation procedures and PEG placement are carried out on-site by an interdisciplinary team in collaboration with anesthesiology and internal medicine. These interventions can typically be performed on a regular ward in a calm and supportive environment.
Our team also provides gene-specific therapies for patients with ALS caused by mutations in the SOD1 gene.
Outpatient care is delivered by physicians specialized in ALS, with regular follow-up visits typically scheduled every 3–6 months.
Appointments
To arrange an inpatient appointment, please contact our case management team:
Phone: +49 (0)731 177-5447, Email: casemanagement.neuro@uniklinik-ulm.de
For outpatient appointments, please contact our patient coordinator Lisa Benz:
Email: lisa.benz@dgm.org
We kindly ask you to complete the questionaire and return it to Ms. Benz.
Please note that a referral from your general practitioner or specialist, as well as any previous medical records, are required for your appointment.
Highly Specialized Care for ALS Patients

In the specialized outpatient clinic for amyotrophic lateral sclerosis (ALS), patients receive comprehensive neurological care. During initial consultations, the diagnosis is reviewed and the individual disease course is assessed. This includes the use of modern biomarkers, such as neurofilament measurements, which can provide information about disease activity.
The consultation also provides time for patients and their families to address urgent questions. Possible treatment options are discussed, including pharmacological therapies, symptom-oriented interventions, and the potential (entirely voluntary) participation in clinical trials.
Another key focus is the provision of medical aids and the prescription of supportive therapies, including physiotherapy, occupational therapy, and speech and language therapy. Respiratory function is assessed to enable early counseling on supportive measures such as respiratory therapy or ventilation, if needed. In addition, nutritional aspects are addressed and social support services are offered. The goal of the clinic is to provide holistic, individualized care that helps maintain quality of life and independence for as long as possible.




As ALS progresses, weakness of the respiratory muscles increases. This can lead to direct symptoms such as shortness of breath, as well as indirect symptoms caused by elevated carbon dioxide levels in the blood, including daytime fatigue, sleep disturbances, impaired concentration, and depression.
In addition, many people with ALS experience problems with airway secretions, such as thick mucus. This can cause persistent coughing and increase the risk of respiratory infections, including pneumonia. Effective treatments are available to manage these symptoms, including mechanical cough assistance devices (“cough assist”) and non-invasive home ventilation using a mask, both of which can significantly improve quality of life.
The respiratory care team at the Department of Neurology, Ulm University Hospital, consists of five specialized respiratory therapists with extensive experience in the care of ALS patients with breathing difficulties. Their responsibilities include:
- diagnosing respiratory impairment (e.g., through overnight carbon dioxide monitoring),
- initiating and adjusting non-invasive home ventilation,
- providing invasive ventilation via tracheostomy in advanced stages of the disease (if desired by the patient),
- supporting secretion management using mechanical cough assistance devices,
- and implementing additional measures to improve respiratory function.
Respiratory care is provided in both outpatient and inpatient settings. The initial setup of ventilation therapy is always carried out in an inpatient setting to ensure optimal adjustment to the patient’s needs.
Respiratory Care Team: F. Krasowski, H. Janeck, F. Ramirez, F. Cekic und F. Boscher






Current standard brain imaging using magnetic resonance imaging (MRI), based on routine protocols and visual radiological assessment, has limitations, particularly in neurodegenerative diseases. Subtle or early changes are often difficult to detect reliably with this approach. In addition, distinguishing between certain forms of neurodegenerative disease can be challenging.
It is likely that specific changes in the brain can only be visualized using novel, specialized MRI sequences. To investigate this further, we examine patients with suspected or confirmed neurodegenerative disease using MRI with innovative imaging methods. In addition to research imaging, these MRI examinations always include all standard images currently used in clinical diagnostics.
The MRI images obtained are evaluated both scientifically and clinically. The results are also made available to the treating physicians to support further treatment recommendations.
Interested or have questions? Please feel free to contact us.
Neuroimaging Working Group, Imaging Center, Ulm University Hospital:
Prof. Dr. Dr. Nico Sollmann, B.A. (Oberarzt Neuroradiologie/Radiologie/Nuklearmedizin)
PD. Dr. Kornelia Kreiser (Sektionsleitung Neuroradiologie)
Prof. Dr. rer. nat. Hans-Peter Müller (Senior Scientist, Radiologie)
Dr. Joachim Strobel (Radiologie)
Benedek Petery (Doktorand Radiologie)

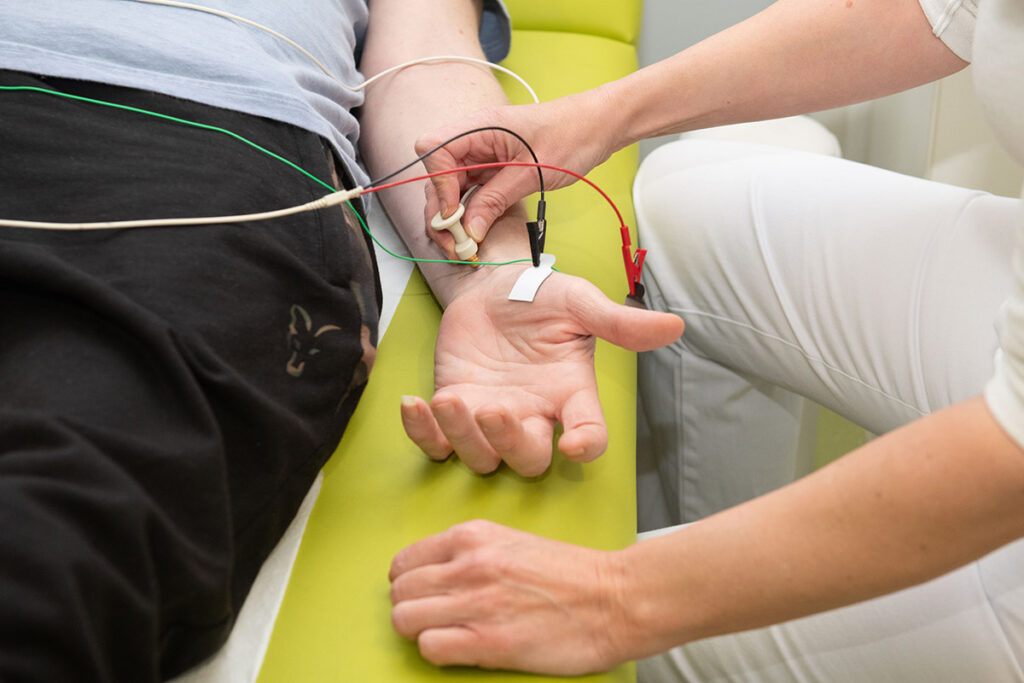
Electrophysiological diagnostics in ALS include nerve conduction studies and electromyography, also known as EMG.
Nerve conduction studies examine nerve function. The nerves are stimulated with brief electrical impulses, and the resulting response potentials are recorded.
During electromyography, a very fine needle is inserted into selected muscles to assess their electrical activity at rest and during muscle contraction.
The aim of these examinations is to identify diseases of the nerves or muscles and to distinguish between them. They therefore support diagnosis, help rule out other conditions, and allow a more precise assessment of the course of a possible nerve disorder.


As part of our interdisciplinary team, occupational therapy aims to enable people with motor neuron disease to live as independently as possible for as long as possible. We work with patients and their families to preserve everyday skills and adapt the home and daily environment accordingly.
We offer functional therapy to maintain joint mobility and help patients make optimal use of their remaining muscle strength. This is important both for managing daily life independently and for facilitating care when support becomes necessary. We are also happy to guide family members where appropriate.



Therapy is adapted to the individual stage of the disease and focuses on the patient’s existing abilities. In this way, we aim to preserve or improve quality of life.
As part of everyday life training, we work on compensatory strategies to help offset lost motor abilities and provide advice on assistive devices. Some assistive devices can be tested during an inpatient stay. Close collaboration with family members is important to us, especially to gain a detailed understanding of the home environment.
To ensure optimal provision of assistive devices for daily life at home or at work, we coordinate closely with medical supply providers.



Almost all people with ALS experience unintended weight loss during the course of the disease, which can have a negative impact on prognosis. This weight loss is caused by hypermetabolism, meaning increased energy expenditure, the exact cause of which is not yet fully understood.
Nutritional therapy in ALS therefore aims to provide sufficient calories using high-energy nutritional sources. Previous nutritional studies, such as the LIPCAL-ALS-I study, suggest that appropriate nutrition may improve prognosis by slowing disease progression.
Based on current scientific knowledge, fats and possibly ketone bodies—either administered directly or through a ketogenic diet—may be particularly suitable.
Our nutrition team consists of specialized ALS physicians, study coordinators, and a dietitian. If you are interested in one of the studies mentioned above or have any questions, please contact:
Elke Fröhlich: elke.froehlich@uni-ulm.de, Tanja Ruschitzka: tanja.ruschitzka@uniklinik-ulm.de

Our department is currently conducting studies on these specific nutritional approaches. These include the LIPCAL-ALS-II study, which tests a high-calorie, high-fat nutritional supplement, and the PEGASUS study, which investigates high-calorie and ketogenic diets in patients receiving nutrition via percutaneous endoscopic gastrostomy (PEG).

The latest genetic methods have led to the discovery of numerous genes in which changes, or mutations, can cause ALS. These genes form the basis of many scientific research projects in experimental and basic research. These discoveries have fundamentally changed our understanding of ALS over the past 10 to 20 years.
In recent years, genetic research in ALS has achieved another major milestone: for the first time, a drug has been approved that directly targets the genetic cause of a small proportion of ALS cases. This drug, the antisense oligonucleotide tofersen, may be effective in patients with a mutation in the SOD1 gene.
Although this treatment is currently suitable only for a small subgroup of ALS patients, it represents a therapeutic breakthrough because it targets the underlying cause of the disease. In other words, in these specific cases, the disease is addressed at its root—the genetic mutation.
This success has led to a shift in thinking and has stimulated numerous additional research projects in university laboratories and pharmaceutical companies. Several further gene-specific therapeutic approaches are currently in clinical development.
It is particularly important that gene-specific therapies are also being developed for patients in whom no mutation in one of the known ALS genes has been identified. The success of the first gene-specific treatment and the prospect of further similar therapies have also changed recommendations regarding genetic testing in ALS patients, as such testing may now have direct therapeutic consequences.
We now also offer genetic testing to patients without a known family history of ALS, as genetic causes can sometimes be found in these cases as well. However, this must always be preceded by detailed and competent counseling. (Neurogenetics Clinic)

Speech and language therapy is a central component of care for people with amyotrophic lateral sclerosis (ALS). Our specialized team supports patients in preserving speech and swallowing functions for as long as possible and in adapting communication options to individual needs.
ALS can affect articulation, voice, and speaking speed. In speech therapy, we help patients improve speech intelligibility, develop efficient speaking techniques, and make the best possible use of remaining abilities. We also provide early advice on supportive forms of communication to ensure a smooth transition to assistive devices if spoken communication becomes more difficult over time.
Swallowing difficulties occur in many people with ALS and may lead to weight loss or an increased risk of aspiration. We perform both clinical and instrumental swallowing assessments and develop individualized treatment plans based on the results. We teach safe swallowing techniques, provide recommendations on suitable food and liquid consistencies, and support patients in decision-making regarding PEG placement.
When spoken communication declines, we provide comprehensive advice on alternative communication options. These include simple aids such as letter boards as well as electronic communication devices and eye-tracking systems. We support patients in selecting, adapting, and training with these aids and work closely with assistive technology providers.
In 5–10% of ALS cases, there is a positive family history, referred to as familial ALS. However, even patients with sporadic ALS, meaning ALS without a known family history, carry causative genetic variants in 10–15% of cases.
Depending on the mode of inheritance, several family members across multiple generations may be affected. Some genetic variants are incompletely penetrant, meaning they do not always lead to disease onset and may skip generations. Some inherited changes can also cause different disease courses or even different clinical syndromes within the same family.
Knowing whether a disease has a genetic cause is relevant for prognosis and increasingly also for treatment, as gene-specific therapies are being approved or clinically tested for a growing number of neurodegenerative diseases.
Genetic testing, particularly predictive testing before disease onset, always requires thorough counseling beforehand. In particular, the potentially serious psychological effects of a pathological finding must be discussed.
The diagnosis of a genetic disease or predisposition can have consequences for the life and life planning of the person affected and their family. It must also be noted that genetic testing does not always provide a clear result. So-called variants of uncertain significance may be found, meaning it remains unclear whether a genetic variant is harmful or benign. This can create considerable uncertainty.
Once the genetic test result is available, the findings and further diagnostic and, where appropriate, therapeutic steps are discussed in person.

The medical care provided by our neuropsychology team focuses on supporting ALS patients and their families and is therefore a central part of interdisciplinary care. Because ALS is a progressive disease that can involve not only motor symptoms but also cognitive and emotional changes in some patients, neuropsychology plays an important role in diagnosis, counseling, and ongoing support.
One focus of our work is the assessment of changes in cognition, including thinking, word finding, and problem solving. As part of comprehensive neuropsychological diagnostics, cognitive functions such as attention, memory, executive functions, and language are assessed.
Some patients experience additional changes that can affect social interaction, such as behavioral changes, reduced impulse control, or impaired social cognition. These changes can be stressful for patients, but especially for families and caregivers. Early recognition is therefore essential—not only to establish the correct diagnosis, but also to provide patients and families with information and comprehensive counseling.
Another focus is psychological support for patients. A diagnosis of ALS represents a major emotional burden and may be associated with anxiety, low mood, grief, and existential questions. Each person copes with the diagnosis differently, and the need for support may arise at different times.
The neuropsychology team offers stabilizing conversations, promotes coping strategies, and supports emotional adjustment to the disease. A central focus is the patient’s social participation and integration. Support is always tailored to the individual needs and resources of the person affected.
The involvement of family members is equally important. Relatives are often under significant strain and increasingly take on caregiving tasks as the disease progresses, which can involve major emotional, time-related, and personal changes. Our team advises families on dealing with the disease, including cognitive and behavioral changes, and offers psychosocial support where needed.
Overall, the aim of the neuropsychology team is to preserve quality of life for patients and their families for as long as possible, reduce stress, and provide holistic support throughout the course of the disease.
We are here to support you.
The Neuropsychology Team

ALS changes many aspects of life. This makes it all the more important that patients feel well supported and understood. Physiotherapy is an integral part of treatment and helps maintain mobility, independence, and quality of life for as long as possible.
At the Department of Neurology, patients with ALS are supported by an experienced and specially trained team of physiotherapists. Therapy follows current medical recommendations and is individually adapted to each patient’s situation.
The aim of physiotherapy is to support everyday movements, such as walking, standing up, turning in bed, or sitting safely. Gentle exercises help maintain mobility and prevent pain, muscle tension, or joint stiffness. Therapists ensure that exercises do not overburden the patient and are adapted to individual resilience.


Respiratory therapy is another important component. It supports breathing, helps with coughing, and can reduce fatigue. Physiotherapists also provide advice on assistive devices, positioning, and movement strategies that make everyday life easier and help conserve energy.
Physiotherapy is regularly adapted as the disease progresses. In close collaboration with physicians and other therapy teams, this provides comprehensive care.
Our goal is to support patients with professional expertise, empathy, and reliability.


In amyotrophic lateral sclerosis (ALS), the respiratory muscles may also become affected over time. Changes in breathing often first occur during sleep and can lead to non-restorative sleep, morning headaches, daytime fatigue, or shortness of breath. Early sleep medicine assessment can help relieve symptoms and improve quality of life.
As a neurological ALS center, we care for many patients in our sleep laboratory and offer diagnostics specifically tailored to ALS.
The most important examination in our sleep laboratory is polysomnography. During sleep, several body functions are measured simultaneously, including breathing, blood oxygen levels, heart rate, brain activity, and muscle movements. This allows sleep quality and nighttime breathing to be assessed precisely. The examination is painless and individually adapted.
If nighttime respiratory weakness is detected, supportive nighttime ventilation via a breathing mask can relieve breathing effort and significantly improve symptoms. Care is provided in close collaboration with our neurological ALS outpatient clinic.
As a specialized center, we are also scientifically active and conduct ALS-related studies in our sleep laboratory. Participation is voluntary and takes place only after detailed information and consent.


